
Everything You Need To Know About the NFHS
The National Family Health Survey (NFHS) is one of the world's largest household surveys, and was launched in 1992. It is widely used to track data on demographic and health indicators across Indian states and districts. In this piece, we explain the history of the NFHS including the changes in its scope and structure, its methodology, its uses, and some debates about the data quality of the NFHS.
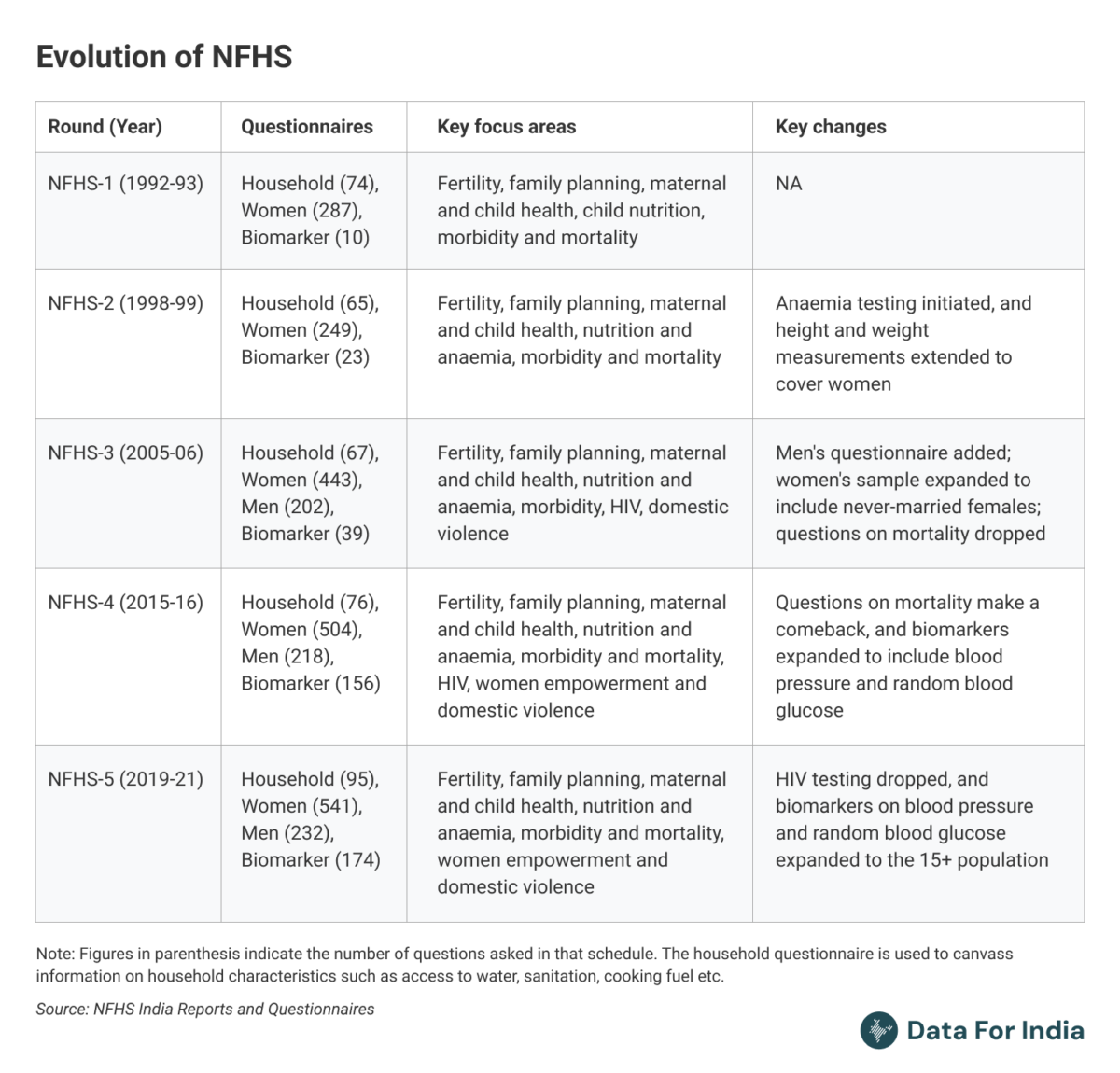
The evolution of the NFHS
The NFHS is part of a global cohort of surveys run by the United States Agency for International Development (USAID) under its Demographic and Health Survey (DHS) program. The DHS surveys began in 1984, replacing two earlier survey cohorts: the World Fertility Surveys (1973-1984) and the Contraceptive Prevalence Surveys (1977-1985), run by USAID across the globe. These surveys were designed primarily to monitor population trends in developing countries.
The first DHS survey in India, christened as NFHS, took place in 1992-93 (NFHS-1). The focus was on generating national and state-level data on fertility, family size preferences, knowledge and practice of family planning, and related topics. It was designed to explore the demographic and socioeconomic determinants of fertility, family planning, and maternal and child health outcomes. The database was intended to assist policymakers and researchers in assessing and evaluating family welfare programmes and strategies.
The survey was conducted under the Indian Ministry of Health and Family Welfare (MoHFW). The International Institute for Population Sciences (IIPS), Mumbai - an autonomous research institute of the MoHFWworking primarily on demography and population health - was designated as the nodal agency for conducting the survey, and state level population research centres were roped in as regional partners to collect the survey data.
NFHS-2, conducted in 1998-99, canvassed information on some of the same topics covered in the first round. Additionally, it included questions relating to the quality of health and family welfare services provided by the government, reproductive health problems, the autonomy of women, and domestic violence.
A men's questionnaire was added for the first time in NFHS-3 (2005-06), covering issues such as family planning choices and health.
In NFHS-4 (2015-16), the sample-size was expanded to provide district-level estimates for key demographic and health parameters. Surveyors used tablets rather than printed questionnaires to collect data in this round, and that speeded up the publication process.
NFHS-5 (2019-21) introduced questions on death registration and disability for the first time.
The NFHS-6 was conducted in 2023-24, but the data is yet to be released. Details relating to the questions asked in this round are available publicly. Questions on disability and biomarker data on anaemia, waist-hip ratio, and waist circumference have been dropped from this round. For the first time since NFHS started, the survey was run solely by IIPS, without any assistance or involvement of USAID.
How the surveys are conducted
Selecting the sample
The NFHS aims to provide representative demographic and health estimates at the national, state, and district levels. Towards that end, it divides each district and state into sub-parts or strata and selects sample villages or urban blocks from them at random.
Once the sampling units (villages/urban blocks) or sub-units are identified, survey field staff are assigned to these units to collect data on housing structures, household type (residential/non-residential) and basic household details (such as household head's name) from all households in that unit. From the list of all households, 22 households are randomly chosen for the survey in a manner that each household has an equal chance of being selected.
This is called a multi-stage stratified sampling strategy, similar to that used by other national surveys.
Conducting the survey
The field staff visit each sampled household and conduct interviews with household heads, eligible women, and men. Each interview team includes three women (who interview female members), one man (who interviews male members), two health investigators (who collect biomedical data such as blood pressure readings and blood samples), and one field supervisor (who conducts on-the-spot data quality checks).
The field staff use mini-notebook computers loaded with a Computer Assisted Personal Interviewing (CAPI) application. They ask questions in a pre-assigned sequence and enter the answers directly in the tablet. This approach, introduced in NFHS-4, replaced the earlier method, where field staff used to note down answers on printed forms. The use of CAPI eliminates the need for separate data entry, reduces manual errors, and incorporates real-time data consistency checks. It also enables the daily transmission of data to the central office, facilitating timely feedback on data quality issues.
NFHS-1 covered over 88,000 households and 89,000 women. The NFHS sample-size was increased considerably from the 4th round onward to ensure representative district-level estimates for maternal, child health, and household characteristics. NFHS-5 covered over 600,000 households, 700,000 eligible women (15-49 years), and 100,000 eligible men (15-54 years). Estimates for men's health outcomes and their family planning choices are computed at the state level only, and require a smaller sample size.
The questionnaire
The NFHS employs four questionnaires: Household, women's, men's, and biomarker.
The household questionnaire, answered by the household head, includes questions on socio-economic characteristics (such as religion and caste) of the members of the household, as well as on access to household amenities (such as source of drinking water and toilet facilities) and assets (such as TV or refrigerator). The data collected on household members from this questionnaire is used to identify men aged 15-54 and women aged 15-49, who are eligible for individual interviews.
The women's questionnaire focuses on reproductive health, fertility choices and related topics. Women aged 15-49 are asked about the number of children they have had (alive and deceased), experiences of miscarriages, abortions, or stillbirths, knowledge and use of contraceptives, and sexual behaviour (number of partners, age at first intercourse etc.). Women are interviewed in privacy or in a separate space to ensure they feel comfortable and can provide honest responses. If privacy cannot be fully ensured, efforts are made to minimise the presence of others, especially men.
The men's questionnaire asks men aged 15-54 about their use of contraceptives, involvement in partner's antenatal and delivery care, and preferences regarding having children.
The biomarker questionnaire is used to record anthropometric measurements such as those relating to height and weight as well as bio-medical data such as haemoglobin levels.
The many uses of the NFHS
India has several demographic and health databases, including the Civil Registration System (CRS), the Sample Registration System (SRS), the Health Management Information System (HMIS), and the decennial census. Among these, CRS and HMIS are incomplete in terms of coverage; census and SRS do not provide individual-level records. NFHS is unique as it not only provides individual records on a regular basis but also provides a wealth of information on health correlates (socio-economic status, healthcare access, and risk factors). This enables researchers to analyse trends, patterns, determinants, and drivers of changes in health outcomes effectively.
Early research using NFHS data centred around fertility dynamics and family planning. However, as fertility levels declined across the country, and public health initiatives such as the National Rural Health Mission (NRHM) gained momentum, the focus shifted to maternal and child health. Researchers have used NFHS data to highlight the persistent socio-economic disparities in maternal and child health outcomes. Poor and socially marginalised households tend to have poor access to health services, and children born in these households tend to fall ill more often, analyses of NFHS data suggest.
Researchers have also used NFHS data to point to the role of institutional deliveries, improved antenatal care coverage, and the adoption of early breastfeeding practices in improving survival odds of newborns in the country. They have also pointed to important non-biological parameters that determine maternal health outcomes such as educational attainment, women's empowerment and male involvement in healthcare decisions.
Research using NFHS data has pointed to the growing prevalence of obesity, diabetes, and hypertension among rural and socio-economically marginalised communities. These conditions are considered as serious risk factors for cardiovascular diseases, and were earlier viewed as a predominantly urban and 'lifestyle' phenomenon.
With the expansion of NFHS' sample-size in the fourth round and the availability of district-level estimates, the database has been used widely to identify regions where welfare programmes need to be targeted as well as to study the impact of those interventions over time. NFHS is also used to track progress on Sustainable Development Goal (SDG) indicators. NFHS also provides the indicators used to compute India's Multidimensional Poverty Index (MPI).
Key debates on NFHS data
Over the years, there have been questions raised and debates over some data in the NFHS, which we discuss in brief here.
Sample size
The six-fold expansion in sample-size in NFHS-4 (to generate district-level estimates) led the National Statistical Commission to express concerns about data quality and comparability with past rounds. The NFHS-4 report acknowledged this issue, stating that "the NFHS-4 figures and those of earlier NFHS rounds may not be strictly comparable due to differences in sample size".
Sex ratio
The NFHS-5 reported a sex ratio of 1,020 females per 1,000 males, which was interpreted as women outnumbering men in India. However, this is not consistent with either the Registrar General of India's (RGI) population projection (the benchmark for population estimates in the absence of census data) or with National Sample Survey (NSS) data. Hence, NFHS data on sex ratios and gender gaps need to be treated with caution.
Unexplained fluctuations in data over time
NFHS data on immunisation has shown inconsistencies, with unexplained fluctuations in full immunisation coverage across states and rounds, as well as an increasing trend in "zero-dose children" (children aged 12-23 months who have not received their first dose of the diphtheria-tetanus-pertussis (DTP) vaccine) in states with relatively better-performing healthcare systems such as Kerala and Tamil Nadu. These trends, unsupported by changes in healthcare delivery, funding, or policy, suggest that data quality issues may be driving these results. Hence immunisation-related findings from the NFHS dataset need to be interpreted with caution.
Similarly, the data on age at death of adults in the NFHS has shown notable inconsistencies, including substantial digit preferences (a bias towards ages ending in 0 or 5), reflecting inaccuracies in reporting. Further, the data indicated significant underreporting of female deaths.
Measurement of anaemia
The NFHS-5 reported a high prevalence of anemia among children and women (with anemia levels higher than in NFHS-4).
The NFHS uses capillary blood samples collected via finger pricks. These are considered practical for field conditions but are likely to produce higher and less reliable estimates than venous samples. The Comprehensive National Nutrition Survey (CNNS) 2016-18 - which used venous blood samples - reported significantly lower anemia among children compared to NFHS.
In March 2024, the WHO released new guidelines recommending the use of venous blood samples and automated hematology analysers in laboratory settings to estimate anemia prevalence. It also revised the hemoglobin thresholds below which a person or child is labeled anemic, lowering the thresholds for children in the 6-23 month age group.
Following the controversy, anaemia measurements have been left out of NFHS-6, and will now be part of the Diet and Biomarkers Survey in India (DABS-I) currently being conducted by the Indian Council of Medical Research (ICMR).
Time taken for the interview
Some researchers have argued that private firms involved in data collection are completing interviews faster than earlier, compromising data quality. However, shorter interview durations in recent rounds may not necessarily indicate compromised data quality. The length of the interview depends on the number of children born in the last five years (repeating sections for each child), and the time needed to ensure privacy protocols for sensitive modules such as domestic violence. Any assessment of variations in interview lengths needs to take these factors into account.
The shift from manual pen-and-paper interviews (PAPI) to automated computer-assisted personal interviews (CAPI) may also have contributed to lower interview times.
Nandlal Mishra, Pramit Bhattacharya (2025), 'Understanding India's National Family Health Survey.' Published on Data for India. Retrieved from https://www.dataforindia.com/nfhs-explainer/ [Online Resource].
This article went live on February third, two thousand twenty five, at nineteen minutes past one in the afternoon.The Wire is now on WhatsApp. Follow our channel for sharp analysis and opinions on the latest developments.



